The Business of Weight-Loss Drugs
Are they all they're cracked up to be?

Introduction
Obesity is an enormous challenge facing modern societies and so the arrival of weight-loss drugs like Ozempic and Wegovy appears to be a good thing. The uptake in the US has been huge, with 8% of adults claiming to have taken them. The rest of the world is following suit. The problem, however, is that not unlike the widespread use of opioids, we are trying to solve a complex issue with a simple solution, and there are plenty of commercial incentives for doing so.
Tackling obesity
It’s important to say before launching into the dangers of obesity that there is plenty of social stigma around it and it’s no one's job to go around judging other people. If you thought the unintentional pun in the first sentence of this piece was the opening salvo of some meanness, you’d be mistaken. The modern world is fundamentally an “obesogenic” environment. Modern “food” is purposefully addictive and non-satiating so we can only talk about personal responsibility up to a point.
That having been said, obesity is a challenge for society. You’d be hard-pressed to look at the evidence and say that it is not a big risk factor for a host of health complications. The biggest challenges the NHS faces now are illnesses related to circulatory problems, musculoskeletal disorders and cancer, which all have strong links to obesity. It’s estimated that around £6.5 billion a year is spent on obesity in the UK.
Pharmaceutical companies
Selling drugs is a business which means they share the same incentives as any other business. People invest in companies to achieve a higher rate of return than they would do by simply putting their money in a bank. That means those companies have to keep increasing their revenue by selling more of something. This is rarely harmless as everything has an environmental impact (clothing) or social impact (social media), but the harms are amplified when we’re talking about health (pharmaceuticals and food).
The most attractive revenue to investors is recurring revenue - it’s why so many companies that sell discreet products have attempted to turn their products into services. Peloton is a good example. They sell exercise bikes but you have to pay a monthly fee to use the app. Selling something once is good, but selling it monthly is even better. Prescriptions are essentially subscriptions and so the pharmaceutical industry has long been motivated to develop drugs which people have to use for a long time.
This got going in the 60s with Valium which Arthur Sackler was successful in marketing to the American public as a cure for anxious wives (see Betty in Mad Men) and indeed any stereotypically female malaise. Ninety million bottles were dispensed annually by the 1970s. Roche, who sold it, didn't bother to do any studies on its addictiveness. By the 1980s everyone realised that it wasn’t doing anyone much good except for Roche and its prescription declined, with the damage it did relatively unclear.
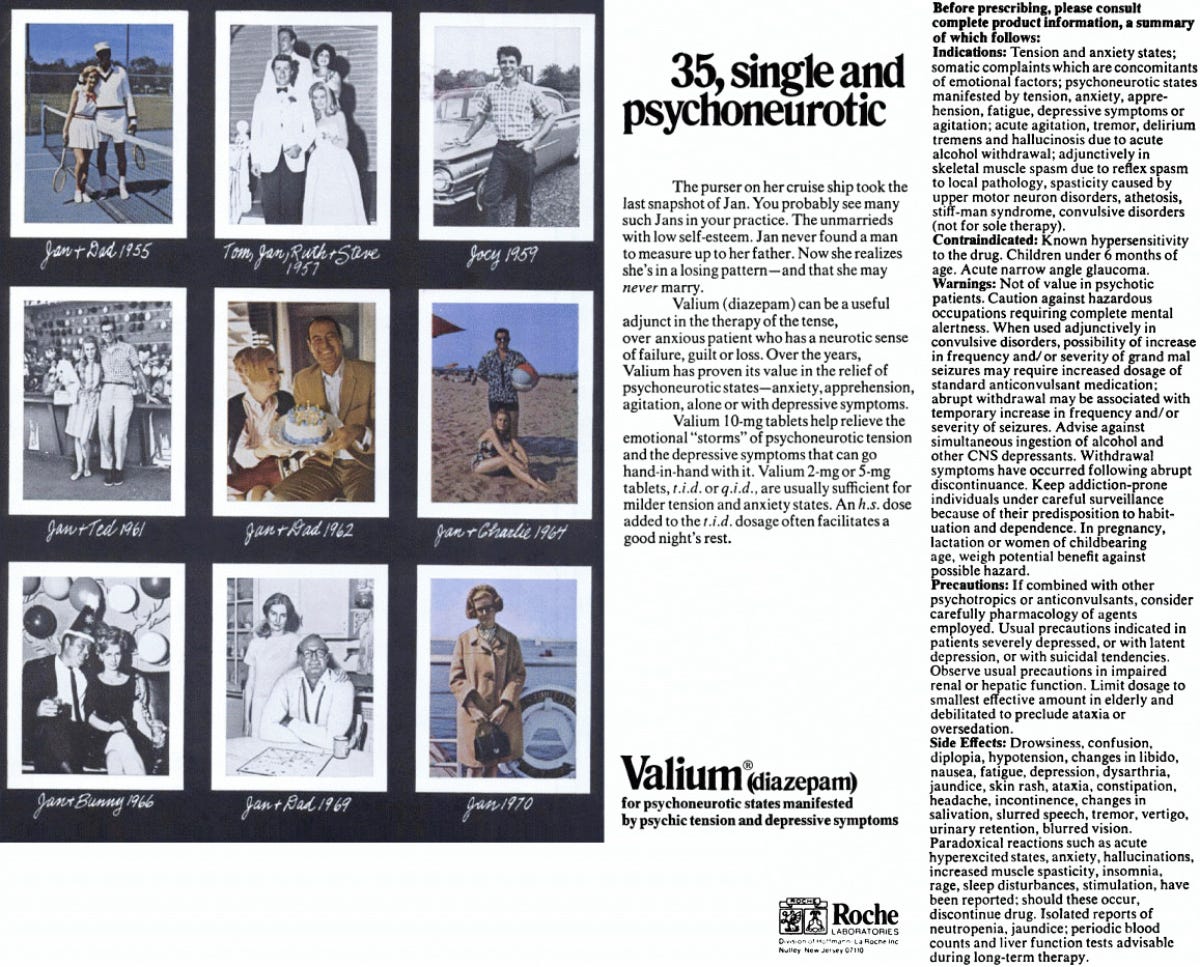
Source: The Open University
Richard Sackler (Arthur’s nephew) recreated the popularity of Valium to an even more devastating effect with the development of OxyContin. The opioid pandemic has been well-documented but it is essentially the story of how Purdue Pharma used a powerful combination of PR and lobbying to convince both doctors and the American public that the solution to any suffering was “pain management” in the form of opioids. This gained immediate traction in much of America’s industrial heartland, where many people had suffered debilitating injuries working in mines and factories.
Pills are appealing to insurers because it’s far cheaper to give someone a prescription for a back injury than a long course of physiotherapy. Purdue also had an army of salespeople motivated by huge performance bonuses to persuade doctors to give their patients OxyContin. Underpinning all of this was support from the Food & Drug Administration, which received help from ex-Purdue employees in developing the pretty lax regulatory framework.
It would be unfair to suggest that this level of cynical profiteering exists across the pharmaceutical industry and when capitalism works well, profit incentives and public good align. Statins, a cholesterol-reducing drug, have been widely prescribed for several decades and have played a role in tackling cardiovascular disease (even if it has been overstated) and provided drug companies with a huge amount of annual recurring revenue. There’s no doubt the majority of people who go into pharmacology are doing it because they want to improve the health of the population. But the fact remains, these are businesses.
In 2022 pharmaceutical companies spent $54 billion on advertising - which is of course only one component of marketing, vast sums are no doubt also spent on public relations and lobbying. It’s illegal to advertise prescription drugs in every country except the US and New Zealand. The impact in the US has been pretty apparent, New Zealand has state-funded healthcare so there’s less of an incentive to dole out pills. There are also only twelve people living there.
Capitalism seems to be the least worst option when it comes to economic systems but we have to remain clear-eyed about the risks when such a strong emphasis is put on profit and growth. We all want to do more and be more, which can have some serious downstream impacts if you happen to be an executive in any large corporation.
Weight-loss drugs
Maintaining momentum after Covid
The pandemic painted the pharmaceutical industry in a largely positive light given the rapid development of the vaccine. Pfizer has even tried to capitalise on the goodwill people felt by launching its direct-to-consumer ‘PfizerForAll’ platform last year. This is currently focussed around respiratory diseases (i.e covid) and migraines but no doubt they will expand their offers as and when they become available.
In many ways, pharmaceutical companies have been in need of that difficult follow-up album ever since the pandemic. Shareholders are never content with a bumper couple of years, momentum has to be maintained. Enter weight-loss drugs, the What’s the Story? (Morning Glory) of pharmaceuticals.
What are these drugs?
Glucagon-like Petide-1 receptor antagonists (GLP-1s) were first approved for use to treat Type 2 Diabetes in 2005. They stimulate insulin creation by coupling with a receptor on pancreatic cells. The benefit for people who are deficient in insulin is self-evident but it was discovered to also have the impact of reducing hunger in individuals (insulin leads to satiation) which in turn leads to weight-loss.
Parallels with the opioid crisis
Clearly a drug that stimulates insulin production is not going to have the societal impact that a psychoactive substance like OxyContin does but there are enough parallels with the crisis that some more thought needs to be given before we charge ahead.
A simple solution
Firstly, like opioids, a weight-loss drug is a simple solution to a complex problem. Obesity is caused by several environmental factors, namely the food we eat and our ability to remain active when we exist in a world of desks, cars and sofas.
The exercise element is a deeply-rooted problem and in many ways no one's fault. I for one am glad (generally) that I don’t have to spend my days foraging for berries and chasing wildebeests. We have to go out of our way to remain active to the level our bodies require. There’s plenty we could do as a society. PE at school seems explicitly designed to put people off exercise forever and cities could be set up better to encourage more active commuting. Standing desks are great for 15 minutes but then they get a bit tedious. On the whole, however, exercise is largely a question of people having the right information and getting on with it.
Food on the other hand is a more insidious challenge, driven by profit. Up until the Second World War food was largely fresh. You had vegetables and you had meat. Tins of stuff had some clear battlefield utility but never really went away again, thanks to their obvious convenience. It was only later in the 20th century that processing food took off to the levels that we see today.
In the 1980s there were several large mergers of tobacco and food companies (Kraft acquired Philip Morris and Nabisco acquired RJR). This resulted in many of the scientists who’d been developing cigarettes turning their hands to developing highly addictive snacks that we still see adorning the aisles of supermarkets today. Alongside there has been a consistent campaign to downplay the adverse effects of sugar, pointing the finger at fat and red meat. Just take a trip to the dairy aisle of your local supermarket and look at how much sugar is in low-fat flavoured yoghurt.
There’s little doubt now about the ill effects of sugar on our health. It leads to weight gain, causes inflammation, impacts our insulin response and is highly addictive. And whenever something is addictive, there is a huge profit incentive. See gambling, drugs (both legal and illegal) and social media. There is every reason for food companies to keep pushing this stuff, they are and it's having a devastating effect on our health. Rather than trying to mitigate this with GLP-1s, the real answer is to tackle the problem itself.
The problems that needed tackling during the opioid crisis were not physical and psychological pain but the underlying issues that caused them from poverty to poor working conditions. Treating the symptoms is never a long-term solution, the problem is that it often makes economic sense for businesses.
Weaponisation of academia
The double-blind placebo trial is held up as the gold standard for academic research. It is the attempt to remove all variables apart from the one you are trying to test. This usually consists of trialling something with one group and not with another and seeing who fares better. When it’s an eczema treatment this works relatively well but when you are talking about multivariate problems like obesity or pain the results are less clear. That’s why it’s hard to prove that eating blueberries definitively increases your lifespan, people who eat blueberries probably also eat broccoli, sometimes go for a run and occasionally chips.
It’s very easy to shape the outcome of a trial depending on the question you are asking and how you present the evidence. Ben Goldacre has documented this incredibly well in his books Bad Science and Bad Pharma. Constructing favourable trials and massaging the results was done extensively to show the efficacy of opioids in reducing pain and it appears there is similar use of academic research concerning weight-loss drugs.
Whether it’s not mentioning the weight gain that happens after people stop using the drugs or pointing to an apparent ability to reduce depression (a study by Nature conversely found a 195% increased risk of major depression), the evidence for their efficacy is far more nuanced than is currently being publicised.
The reality is that it is far too early to say anything definitively either way but we have to be careful about the current narrative which suggests that governments have almost a moral imperative to distribute these drugs as quickly as possible. Even worse there is a whole black market now at work, selling knock-off versions through social media. We have not exhausted all other avenues for tackling obesity and until we have we need to tread carefully with widely prescribing drugs that at best might be ineffective in the long term and at worst, dangerous.
A panacea to solving all our health problems
OxyContin was originally used for the treatment of pain in the context of cancer, which can of course be extreme and patient comfort is often as important as treating the underlying issue. Minutes from a Purdue Pharma marketing team meeting revealed how they explicitly targeted family physicians to “expand the use of OxyContin beyond cancer patients to chronic non-malignant pain”. This ultimately saw strong opioids being prescribed for every sort of pain, and we humans are pretty predisposed to feeling pain.
GLP-1s were initially used to treat diabetes which was expanded to weight loss. In the past year or so they’ve been proposed as a potential treatment for substance abuse, intestinal diseases, asthma and Alzheimer’s. Miracle drugs are not without precedent, antibiotics transformed healthcare in the first half of the 20th century. Generally however, a healthy dose of scepticism is required about such wide-ranging claims.
Conclusion
Weight-loss drugs are not opioids. They are not addictive and do not have the acute risks that strong painkillers do. We are however in a situation where there are several conflicting incentives at work and there is a serious risk of long-term damage to society from short-term thinking. As with all deep-routed and complex problems, there is no silver bullet. This has ever been the case and we would do well to learn from the past and act accordingly.